Your written narrative will demonstrate your readiness to practise against the five Good Scientific Practice domains by directly referencing completed evidence in your portfolio. You will need to demonstrate that you recognise your current stage of ability as well as your continuing development needs.
In summary, the written reflective narrative of the IACC assessment requires you to:
- Analyse your completed evidence in your portfolio.
- Synthesise what you have learnt against the five Good Scientific Practice (GSP) domains:
- Professional practice
- Scientific practice
- Clinical practice
- Research, development and innovation
- Clinical leadership
- Reflect on gaps in knowledge and practice.
- Demonstrate a plan of action to inform future practice and development.
Writing your reflective narrative
Critical reflection involves a process of thinking which demonstrates your ability to:
- explore, question, and analyse your experiences
- apply your knowledge
- use your knowledge to enhance your understanding of these experiences
- use your knowledge to shape your future experiences
- learn from past experiences and implement changes to ensure ongoing professional development
You are required to use the “what? so what? and now what?” model of reflection (Driscoll, 2007) to write your narrative. This model is summarised below:
Driscoll Model of Reflection
Driscoll, J. (ed.) (2007) Practicing Clinical Supervision: A Reflective Approach for Healthcare Professionals. Edinburgh: Elsevier.
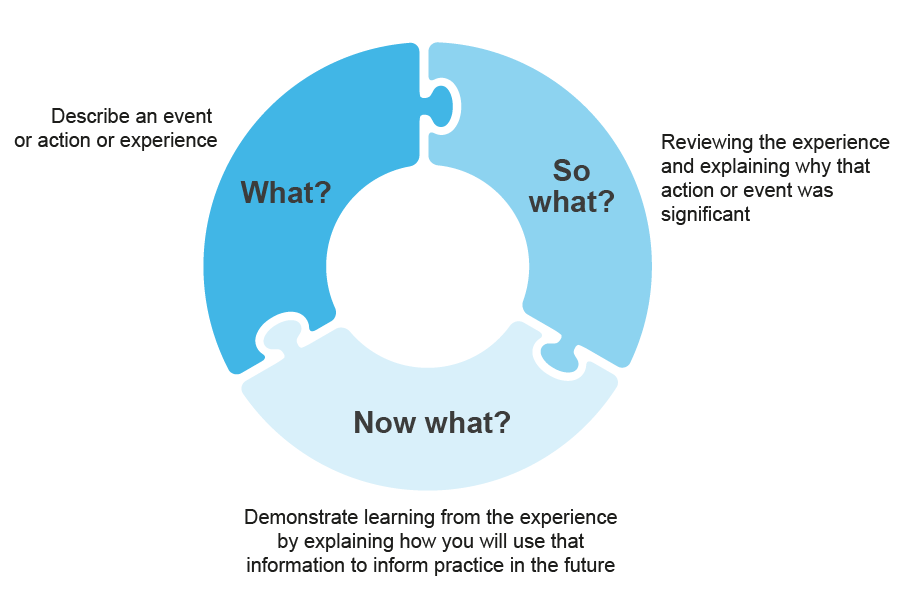
Content of the graphic 'Driscoll Model of Reflection'
What?
Describe an event or action or experience
So what?
Reviewing the experience and explaining why that action or event was significant
Now what?
Demonstrate learning from the experience by explaining how you will use that information to inform practice in the future
Using the Driscoll model for the IACC reflective narrative
What?
You will briefly describe the evidence from your portfolio which demonstrates your readiness to practice for each of the five Good Scientific Practice domains.
So what?
Reflective pieces will build on descriptions to analyse and unfold the account further. You will analyse the evidence you have referenced.
- What does it prove?
- How do you feel about the evidence and the experiences?
- What are the gaps in your knowledge?
Now what?
Critical reflective pieces will assess your own capabilities (knowledge and skills) and further learning needs or support. This is where you will demonstrate that you are a lifelong learner and that you can critically evaluate your practice.
- What are you going to do about the gaps in your knowledge or practice?
- How are you planning to develop further?
Examples of "what? so what? and now what?"
The examples listed below are from IACCs which passed. You can identify good practice for example, they are clearly referenced to evidence in the portfolio, but they also use the “what? so what? now what?” model of reflection.
After each example an illustration is given on how it reflects Driscoll’s approach to reflection but remember when writing your IACC it must be presented in a continuous narrative following the template and guidance.
Complete examples of the five domains
The following examples are from trainees who successfully passed their IACC. All references to the trainee and location have been removed.
publications